
日本語 Japanese, Français, English, Italiano, Español, Deutsch, Português
The Kuriki method (the first edition in 2007) is a theory about Tourette’s syndrome (tic disorder) and obsessive-compulsive disorder to cure these diseases without medication. This theory is based on the author’s inference and interpretation regarding the structure of these diseases. Since it has been written for the psychoanalysts, reading will be difficult for people in general and it might be sometimes read erroneously. Therefore the Kuriki method must presuppose that the patient is treated by a nearby psychoanalyst, and that, between the patient and the Kuriki method, there is always the psychoanalyst. In the broad spectrum of autism spectrum disorders, for some patients, the disappearance of a neurotic bodily symptom can be harmful to their fragile psychological balance. The explosion of emotional catharsis, which has strong repercussions, is done only for three seconds, once a week: beyond this rhythm, it would be an accident caused by negligence, and the psychoanalyst who is inexperienced in emotional catharsis must take responsibility for the temporary mental collapse caused by the accident. Also, to the patient who has weak capacity of logical reasoning, the psychoanalyst must explain well on the violent emotion of revenge caused by the illusory confusion between the person of the traumatic image in his head and the person in the real world.
Cure for Tourette’s syndrome (tic disorder) and OCD without medication
§31
The lower layer
Encapsulation
The traumatic emotion is enclosed in the capsule of insulator in a state of potential emotion. The image, which is on the surface of the mass of emotion, is classified in the memory in the same way as ordinary images, which have no emotion, and cannot be recognized as a traumatic image. Consequently, the patient thinks he has forgotten the trauma, or else he thinks he has no trauma. In fact, the traumatic image is always visible. As it is visible, it can be avoided. The means of preventing the traumatic image is the triangle of the upper layer.
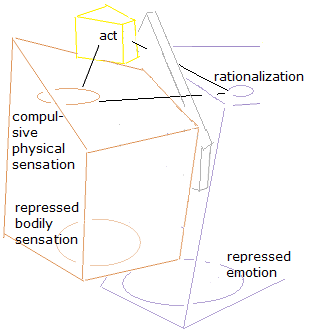
The upper layer of tic disorder is a small triangle that consists of three sides of relationships.
They are the relationships between
(1) rationalization and intention,
(2) the « compulsive intramuscular sensation » of tic disorder and intention,
(3) rationalization and the « compulsive intramuscular sensation » of tic disorder.
(1) The rationalization-intention line passes through the Super-ego. The rationalization selects a voluntary movement that can be easily justified and the psychic motor unit of voluntary muscles that corresponds to this movement. The manner of tic movement is determined by rationalization with precision and enters the Conscious. The precision is remarkable, above all, in the pronunciation of words of coprolalia, the movement of spitting tic, the movement of clapping hands tic (with both hands), etc., which contrasts with the real, involuntary and uncoordinated muscle contraction of dystonia.
(2) In the structure of the disease of tic disorder, the intention yields to the Absolute-Compulsion. In the Conscious of the patient, the intention yields to the « compulsive intramuscular sensation » of tic disorder. The intention is forced to do a voluntary movement of the tic movement as the resolution of the « compulsive intramuscular sensation » of tic disorder, which amplifies itself in the muscle towards the saturation of the necessity.
(3) Direct relationship between the Unconscious and the body.
The line between the « compulsive intramuscular sensation » of tic disorder and the rationalization does not pass through the Superego. The libidinal energy produces the « compulsive intramuscular sensation » of tic disorder in the voluntary muscle that has been selected by the rationalization. In contrast to phobia, in which about 10 seconds are needed for the effects of adrenaline fulfill, such as fear of change in bodily condition, double fear of fear of the increase of change in body condition, the amplification of the sensation of urgency, in tic disorder, the Libido is directly related to the selection of a voluntary muscle by the rationalization. The « compulsive intramuscular sensation » of tic disorder is produced in the voluntary muscle in electric speed. The « compulsive intramuscular sensation » of tic disorder is not made by adrenaline secretion. The direct relationship between the Unconscious and the body at libidinal level is a central element of the structure of neurosis.
The presence or the absence of the psychological trauma
While the onset can be at a very young age, a tic disorder does not start only with the upper layer, without lower layer. Often patients with tic disorder have another neurotic upper layer, such as obsessive-compulsive disorder, and the presence of the common lower layer, which is the cause of the Absolute- Compulsion is inferred. The patients who consider that they have no sexual or genital psychological trauma do not need to think about the presence or the absence of the psychological trauma. This discussion is not necessary for the patients with tic disorder. The patient who thinks that he has no trauma does not need to change his mind. Only with the awareness frequent of disagreeable bodily sensations of the upper layer, automatically, the trauma will starts to be visible gradually in two or three weeks. The upper layer covers the lower layer, thus, the decomposition of the upper layer will make the lower layer visible. The understanding of the upper layer provokes automatically the discovery of the sexual or genital trauma.
Irreversibility of the Kuriki method
In this sense, it seems that, once started towards healing, the treatment of the Kuriki method cannot go back and cannot stop until the completion of the healing.
In this regard, there are three possibilities.
· If no trauma is visible, it means that the Kuriki method does not work.
· If the trauma has been found, the patient should clean this trauma for the life to come.
· Patients often have a false memory; false trauma, which is different from reality. This is one of the roles of the psychoanalyst. While the real traumas of tic disorder are due to childish susceptibility to normal things in everyday life, the false traumas are errors of memory, such as sexual abuse; caution should be exercised. False memory is a problem of psychoanalysis as a whole; it is beyond the area of responsibility of the Kuriki method only.
Catharsis
In fact, tic disorder cannot be cured automatically by the discovering of the traumatic image. Without intentional emotional catharsis, which is done little by little, the treatment of tic disorder does not advance. If the patient does not want the treatment with the Kuriki method any more, only stop doing the emotional catharsis can interrupt the healing. The patients with tic disorder have strong function of repression, and intentional catharsis is indispensable for the treatment.
The Kuriki method requires three adventures.
· When the sexual or genital trauma has been found, the patient will be able to forgive rationally the person who is responsible for this trauma? the patient will not be violent toward this person? Cf., §08.
· Is the patient capable to do emotional catharsis little by little? Abreaction is powerful. The patient mustn’t despise its effects. Cf., §35.
· In the process of healing, when the patient has a transitory feeling of anxiety, which is caused by a temporary loss of mental balance, is he or she able to wait calmly and objectively the recovery? (10 minutes?) Cf., §35.
The adventures in the Kuriki method are risks of the Kuriki method: they are also worries of the author. The author clearly writes that emotional catharsis should be done with the help of a psychoanalyst in your neighborhood.
Summary Introduction 01 02 03 04 05 06 07 08 09 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35 36 37 38 39 40 41 42 43 44 45 46 47 48 49 50 [pdf] [Appendix; A classical therapy for panic disorder and phobia] [Donate to the author]